Loss of Pulse Detection on the Google Pixel Watch 3
March 20, 2025
Kamal Shah and Jake Sunshine, Research Scientists, Google Research
Loss of Pulse Detection on Pixel Watch 3 can detect loss of pulse and automatically place a call to emergency services, potentially saving lives. Here’s how we created and tested this feature.
Quick links
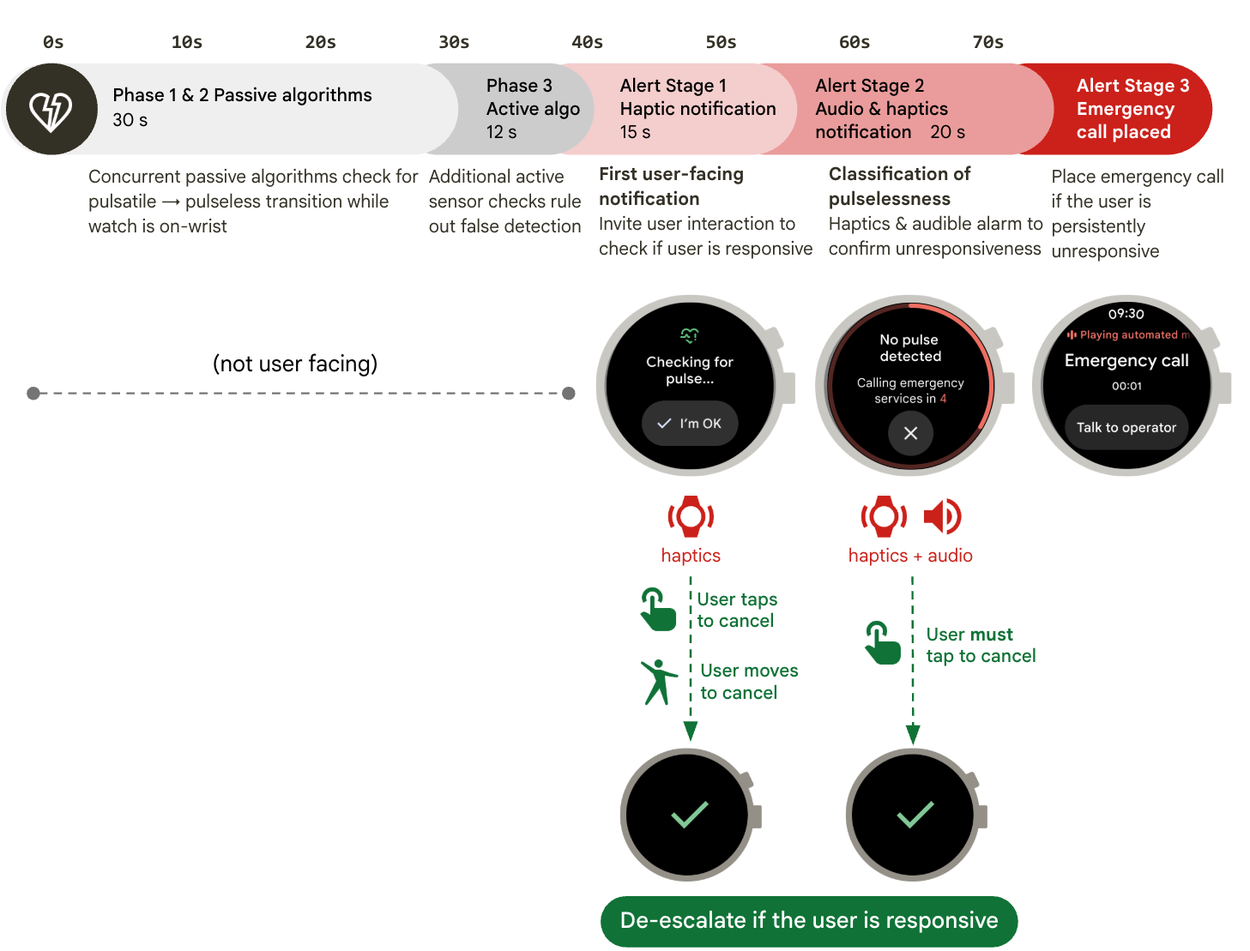
Unwitnessed out-of-hospital cardiac arrest (OHCA), when an individual experiences a pulseless arrhythmia without nearby bystanders who could activate an emergency response on their behalf, is a seemingly intractable public health challenge. OHCA leads to millions of deaths worldwide, and it is estimated that one half to three quarters of victims experience these events in unwitnessed settings. About half of unwitnessed OHCA victims receive no resuscitation because they are found too late and attempted resuscitation is determined to be futile. The time-sensitivity of these events is reflected by the tremendous societal investments we make to minimize the time from collapse to resuscitation as part of the “Chain of Survival” standard of care, for example through cardiopulmonary resuscitation (CPR) training, public access defibrillation, and community responder programs. All of these investments, however, do not address the fundamental challenge of unwitnessed OHCA — they are predicated on bystanders observing events and activating emergency responses.
In “Automated loss of pulse detection on a consumer smartwatch”, recently published in Nature, we provide evidence for a new paradigm of OHCA detection deployable on a mass market wearable device, creating an opportunity to transform unwitnessed events into functionally witnessed ones. We show that a smartwatch algorithm can opportunistically detect the cardinal sign of OHCA, loss of pulse, with a performance profile that enables societal implementation, with appropriate sensitivity and a low frequency of errant calls. In this blog post, we describe how we built and tested the algorithm on a consumer smartwatch.
The standard of care, the “Chain of Survival,” relies on timely identification, which until now required a human witness.
The power of witness status
Witnessed OHCA events have a substantially higher (7.7×) survival rate than unwitnessed events, attributed mainly to bystander presence. Bystanders play a crucial role in improving outcomes by recognizing the emergency, contacting emergency medical services (EMS) promptly and, in some instances, providing earlier resuscitation. For every minute people go without resuscitation, chances of survival decrease by 7–10%, underscoring the enormous prognostic role of time. As a concrete example, in Seattle/King County, WA, witnessed OHCA has a 20% survival rate whereas unwitnessed events have a 4% survival rate. From an epidemiologic perspective, an intervention that reduces mortality by a significant 16% (absolute difference) presents a considerable opportunity to improve health outcomes. Conceptually, viewing witness status as a theoretical intervention, converting an unwitnessed event to a witnessed one could equate to a number needed to treat (NNT) of 6 people to save 1 life — a highly favorable potential benefit profile from a public health intervention standpoint as long as false detections can be minimized.
How Loss of Pulse Detection works
The Loss of Pulse Detection feature has a multimodal algorithm that runs passively on a consumer wearable, consuming data from onboard photoplethysmography (PPG) and accelerometer sensors
Given the rarity of loss of pulse events and the consequential impact of errant calls from false positives, the algorithm consists of multiple gates that must be passed before a classification is made:
- A sudden large drop in the alternating current (AC) component of the green PPG, suggestive of a transition from pulsatile to pulseless state, accompanied by concomitant stillness in the accelerometer.
- A machine learning algorithm, trained on a diverse set of users, that uses data from the PPG and accelerometer that quantifies the probability of a pulsatile to pulseless transition (more below).
- Additional sensor checks to confirm that a weak pulse is absent by using additional LEDs and photodiodes with different geometries, wavelengths, LED currents, and photodiode gain settings.
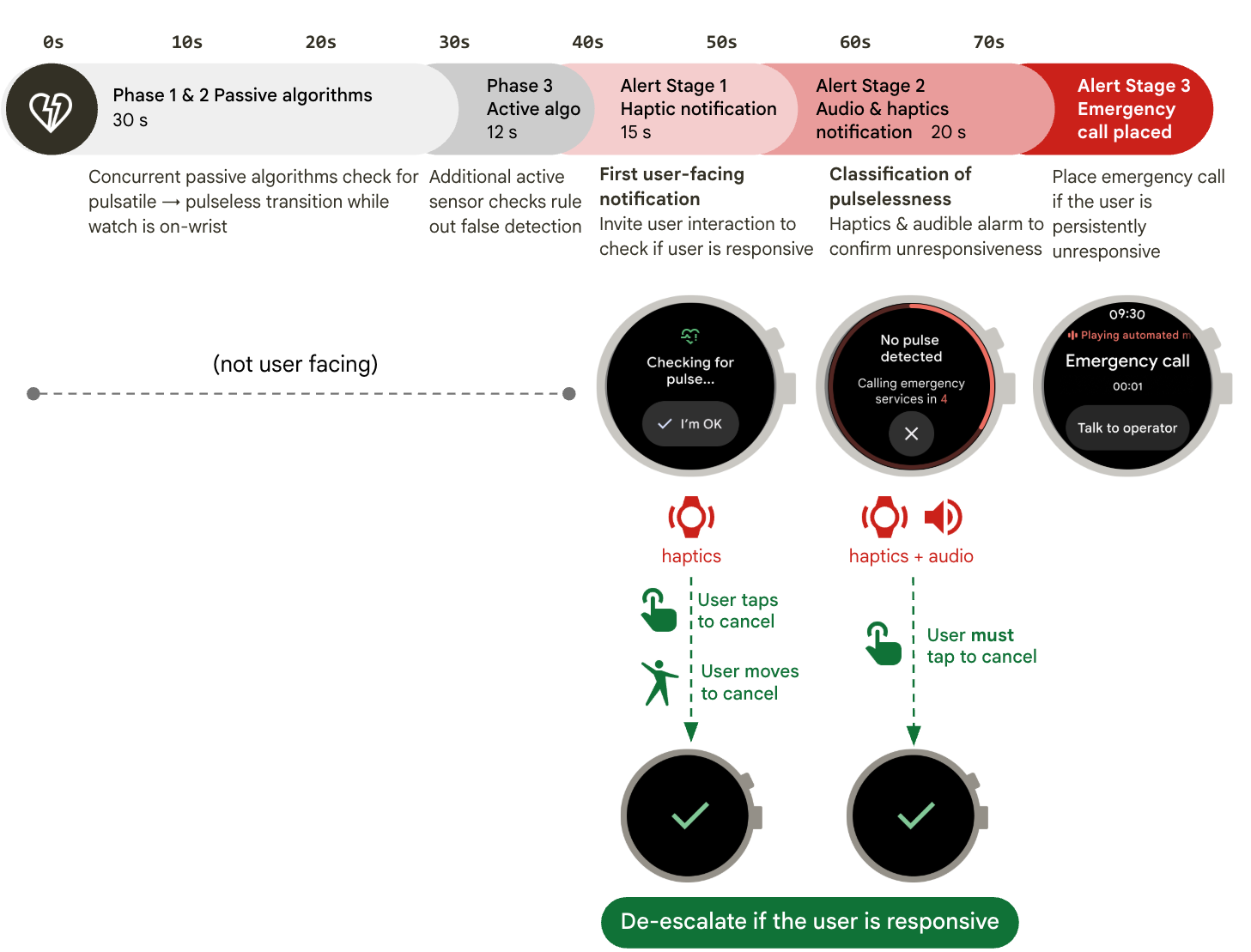
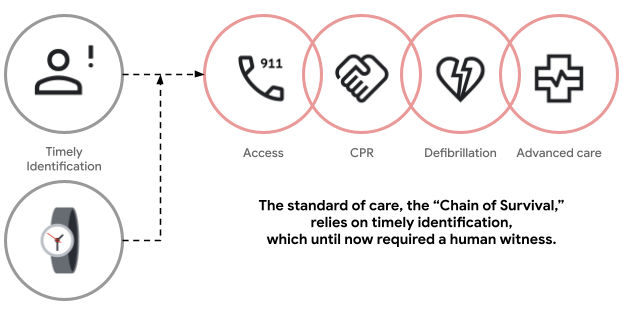
If all three sequential gates are met over a short period of time (designed to detect events in less than a minute), then the feature will check for responsiveness. The feature does this with two check-in prompts that consist of visual, haptic, and audio notifications. If the user remains persistently unresponsive, suggesting a potential true loss of pulse event, then the watch will attempt to contact emergency services, providing information on the situation and location of the user. To minimize the risk of errant calls, the algorithm provides the user with an opportunity to de-escalate if they move their arm purposefully, under the assumption that responsiveness is inconsistent with the physiological state of true pulselessness.
A timeline of the Loss of Pulse algorithm detection sequence illustrates the algorithm stages that can lead to the placement of an emergency call.
Example of the user flow for the Loss of Pulse Detection feature. An animation of the Loss of Pulse Detection feature in action on Pixel Watch 3. First, the watch face shows text saying the watch is checking for a pulse, above a button the user can tap that says I’m OK. If the user doesn’t respond, the watch shows a countdown and places a call to emergency services.
Algorithm development
Building a loss of pulse detection algorithm faces several challenges. These events are life-threatening and rare, meaning we cannot assemble a cohort waiting for events to occur, since it would take millions of person-years to capture hundreds of events prospectively. We overcame this challenge by partnering with cardiac electrophysiologists and their patients. Specifically, we had people who had previously scheduled testing of their implanted cardiac defibrillator wear a watch while their heart was temporarily stopped during this defibrillator test. This allowed us to safely collect data from people with a pulseless arrhythmia, ventricular fibrillation, prior to their defibrillator shocking them back into a pulsatile rhythm. Our key insight was that the pulse signal at the wrist looks similar if the heart stops (like in the electrophysiology lab) or if you occlude the arterial blood supply to the wrist using a pneumatic tourniquet (which is more efficient and safer to reproduce), shown in the figure below. This foundational insight enabled us to scale data collection using arterial occlusion with diverse participants and build an algorithm that we could then test prospectively.
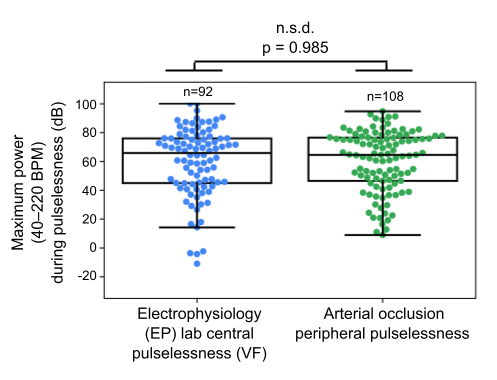
A box plot overlaid with a jitter plot that compares pulselessness observed in a cardiac electrophysiology lab and with arterial occlusion. There is no significant difference in the maximum power of the power spectrum at typical pulse frequencies between central pulselessness observed in a cardiac electrophysiology lab and peripheral pulselessness induced with arterial occlusion. This foundational observation enabled us to develop loss of pulse detection algorithms on arterial occlusion pulseless data.
After we implemented the Loss of Pulse Detection algorithm on a watch, we conducted multiple studies to test the algorithm. First, we performed two studies that verified that the algorithm had minimal false positives. We had hundreds of participants wear the watch during their everyday activities. We found that there were minimal false positives: only 1 errant call in over 21 person-years of wear time. Next, we verified that the algorithm detected loss of pulse events in two additional studies. We found that the algorithm was sensitive in participants who simulated common loss of pulse event scenarios, such as those that occur during sleep or are accompanied by collapses. All four studies included participants of diverse age, sex, and skin tone, demonstrating that the algorithm could work for a broad representation of users.
How Loss of Pulse Detection is built responsibly
Our foremost priority when designing Loss of Pulse Detection was to ensure that the feature had clinically meaningful performance, contextualized for the status quo of unwitnessed events, which are nearly unsurvivable, and was appropriate for deployment at societal-level scale.
Building responsibly to minimize false positives
The two post-algorithmic, pre-phone call check-in gates help minimize unintentional calls by giving users an opportunity to de-escalate if they are indeed responsive. In one prospective clinical validation study, we found that in the 16 instances in which the pre-phone call check-in gates were shown, all but one (94%) were cleared by responsive users. The design of the first-check-in stage (which consists of a visual notification and strong haptics) facilitates de-escalation by clearing via button tap or purposeful motion, such as by rotating the wrist. Individuals who are unresponsive to the first check-in are shown a second, more noticeable notification, which is accompanied by an audible sound in addition to haptics. Only individuals who are persistently unresponsive for 35 seconds proceed to the next stage where the watch attempts to place an emergency call.
In many countries, emergency calls are first triaged by public service answering points (PSAPs), which involves trained individuals who forward time-sensitive emergencies to appropriate professionals. For example, suspected cardiac arrest cases often warrant emergency medical services (EMS) dispatch. The Loss of Pulse Detection feature provides essential context to PSAPs and EMS by describing the nature of the potential emergency (suspected loss of pulse and unresponsiveness), location, and the detection method (by a wearable). The nature and content of this message was informed by our conversations with EMS stakeholders across North America.
We didn't want skin tone to be a barrier to using the feature and we worked hard to ensure it is not. We ensured our training and validation data were representative of the broader population and designed the algorithm deliberately to help ensure the sensitivity of the algorithm did not appreciably differ by skin tone.
Practical implementation on a wearable
Smartwatches constrain the memory, power, and network connectivity available to passive algorithms, mainly to maximize battery life. These constraints informed the design of the Loss of the Pulse Detection feature: the first algorithm stage uses data from sensors that are typically already activated, including the green PPG for heart rate and accelerometer for step counts. Subsequent algorithm stages opportunistically activate additional PPG channels if a potential loss of pulse event is detected. This multistage, multimodal design ensures that the feature minimally impacts the watch’s battery life even though the end-to-end algorithm runs entirely on the watch.
Conclusions
We intend the Loss of Pulse Detection feature to provide a new paradigm for opportunistic detection of unwitnessed loss of pulse events. Given the enormous difference in survival rates between witnessed and unwitnessed cardiac arrests, deployed at scale, such a system may present a significant opportunity to help improve outcomes in unwitnessed circumstances. We hope that Loss of Pulse Detection on consumer wearables can provide public health benefits for individuals who experience unwitnessed loss of pulse events and help get them evidence-based resuscitation faster.
Acknowledgements
The research described here is joint work across Google Research, Google Health, Google DeepMind, and partnering teams, including Consumer Health Research, Personal Safety, quality, regulatory, and clinical operations. The following researchers contributed to this work: Kamal Shah, Anran Wang, Yiwen Chen, Jitender Munjal, Sumeet Chhabra, Anthony Stange, Enxun Wei, Tuan Phan, Tracy Giest, Beszel Hawkins, Dinesh Puppala, Elsina Silver, Lawrence Cai, Shruti Rajagopalan, Edward Shi, Yun-Ling Lee, Matt Wimmer, Pramod Rudrapatna, Thomas Rea, Shelten Yuen, Anupam Pathak, Shwetak Patel, Mark Malhotra, Marc Stogaitis, Jeanie Phan, Bakul Patel, Adam Vasquez, Luke Walcher, Christina Fox, Alistair Connell, Jim Taylor, Jacqueline Shreibati, David Miller, Daniel McDuff, Pushmeet Kohli, Tajinder Gadh, and Jake Sunshine. We are grateful to Flo Thng, John Hernandez, Michael Howell, and Karen DeSalvo. We are also grateful to the study participants who made this research possible.
-
Loss of Pulse Detection may not detect every instance of a loss of pulse and is not intended for users with pre-existing heart conditions or those who require cardiac monitoring. It does not diagnose or treat any medical condition or provide follow-up care. Emergency calling is dependent on call functionality, such as your phone or watch being charged and having adequate cellular connectivity.
-
Labels:
- Health & Bioscience
- Mobile Systems
- Product
Quick links
Other posts of interest
-

March 17, 2026
Google Research at The Check Up: from healthcare innovation to real-world care settings- Health & Bioscience ·
- Machine Intelligence
-
March 17, 2026
Improving breast cancer screening workflows with machine learning- Health & Bioscience ·
- Human-Computer Interaction and Visualization
-

March 11, 2026
Exploring the feasibility of conversational diagnostic AI in a real-world clinical study- Generative AI ·
- Health & Bioscience ·
- Machine Intelligence

